

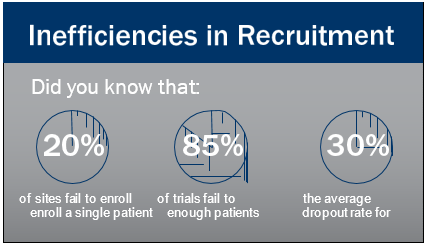
Each day that a drug development program is delayed costs the sponsor $600K to $8M in potential revenue, according to Industry Standard Research. Enrollment and retention inefficiencies (see below) are the primary drivers of delays. As studies have become more complex, the burdens on the patient have increased, deterring participation.
Everyone benefits when study designs factor in the special needs of patients. The sponsor reaches enrollment targets quickly and at less cost. The patient experiences fewer difficulties during the trial and is less likely to drop out. The burdens on the site are reduced. The trial is more likely to be completed on time and at less cost. Three types of patient retention tactics can overcome a range of common barriers to clinical trial participation.
THE CHALLENGES OF RARE DISEASE TRIALS
Rare disease trials, with their scarce population of geographically-dispersed patients, often require long- distance travel. Finding volunteers from a small pool to follow protocols that require long-distance travel, overnight stays, and disruptions to daily routines is a tall order.
When the trial participants are children, another layer of complexity is added. Indeed, 50 percent of people affected by rare diseases are children, according to Industry Standard Research. The trial burden for a child extends to the parent(s) to make the decision to enroll, to arrange for days off from work, and to travel with a potentially ill child.
Scientific American recently reported the results of a Harvard University study that found more than 40 percent of pediatric clinical trials were never finished or were completedbutnotpublished, evenfiveyearslater. The Harvard team discovered the biggest reason for study failure was an inability to attract enough children to participate.¹
Regardless of the age of study patients, failure to offset the burdens of participating in a trial can result in enrollment delays, extended study time, and even a failed study. It is more cost-effective to address potential enrollment challenges in study design and operational strategy, rather than wait for enrollment challenges to occur when the cost of study sites and their multiple human resources must be extended.
The good news is this new approach of incorporating tactics to remove controllable barriers to patient participation is showing great promise.
3 PATIENT RETENTION TACTICS TO OVERCOME TRIAL PARTICIPATION CHALLENGES
1. Patient Travel Services
Imagine the burden for the patient who has to travel for study participation. Patient travel services can be highly customized to meet the needs of each individual. The ultimate goal is making the travel as effortless as possible for the patient.
How do travel services work in a clinical trial?
Currently, my team is managing travel services to support a pediatric multiple sclerosis trial across the United States and Europe. Door-to-door travel service is provided for the patients and their parents who are required to travel long- distances. The participants are children with a relapsing form of multiple sclerosis. Over the course of the study, a patient may be perfectly well, or at any given time he/she could relapse. Parents must consider the burden of travel requirements on their child’s schooling and their own work commitments. That is a potential barrier to both enrollment and retention. Therefore, the sponsor has arranged for a service to take the family from the doorstep of their home to the study site and back.
One Patient’s Experience
One patient lives in Belarus, where weather conditions can be extreme. The child and parents must leave home at around 5 a.m. in minus 23ºC weather, to arrive for a mid-morning site visit. As part of the door-to-door travel service, a driver greets the patient’s family at their home for pickup. The same driver transports the family for each visit, to build a level of comfort and familiarity. The driver then takes the family to the train station. Another driver picks them up and takes them to the research site. A local travel coordinator is provided as a contact at the destination to support the patient’s family as they travel. If any questions arise, or plans change, the family can speak to the driver of their car, or to the local travel coordinator, who can assist them on their journey.
Travel worked great! Very easy. I will be using this service for this particular patient for the next year. Thank you for your service.
—From Principal Investigator
One Patient’s Visit Challenge
In another example from the same study, one participant is 17 years of age. Normally, this patient travels to the study site with parents. But, on one particular occasion, the parents were not able to travel with the patient due to work commitments. Yet because the travel routine was very familiar to the patient (e.g., same driver and familiar route), the parents were comfortable allowing the patient to travel without them from home to the study site. Without the travel support, this patient would not have made the site visit, potentially delaying the visit or causing the patient to drop out.
Eliminating Financial Barriers
Another potential barrier is the financial burden of the cost of travel. A simple solution for handling travel expenses is to issue each participant a payment card for their use during the study. Before every study visit, the card is preloaded with an agreed upon amount. The amount is determined by an ethics committee and can differ from country to country. The preloaded card removes the burden of filing expense- related paperwork or waiting for reimbursement.
Scalability Of Travel Services
Concierge travel services can be scaled for one patient or hundreds. An online portal or patient questionnaire can capture individual travel requests. With large numbers of patients, the cost-saving benefits of meeting recruitment and retention timelines are magnified by the number of patients using the service.
2. Home Health Nursing Services
In the typical clinical trial model, patients travel to investigator sites for study visits and administration of the trial drug. Home health nursing services take the study to the patient by offering nursing visits in the patient’s home. The convenience and care provided by registered nurses can help compliance among study participants with special needs, like pediatric patients, those who are too sick to travel, patients with mobility challenges, and those who live far from the study site.
Engaging registered nurses to take the trial to the patient’s home removes the significant burden of asking the ill patient to travel. Home care nurses can perform a variety of clinical trial support services, including:
• study drug transportation, preparation, and administration
• injection training
• blood and other specimen collections
• data and complex laboratory specimen collection and processing
• coordination of specialty courier shipments
• assessment and adverse event collection and reporting
• clinical assessments
• questionnaires
• compliance reviews
• post-study drug observation
• study drug accountability
• patient education, by phone and in-person
• patient consent
In-home nurses can also support trials by offering emergency support for patients who are staying in a hotel during their trial.
Case Study: One Sponsor’s Need For Emergency Nursing Services
Clinical trial nursing services were needed to support a Phase 3 rare autoimmune disease trial. As with many rare disease trials, ensuring that enrolled patients completed study requirements without loss-to-follow-up was crucial. The study was designed to assess the efficacy and safety of the study drug compared with placebo in adults who had been receiving the study drug via a separate open label trial.
Patients enrolled in the open label trial who consented to be enrolled in the Phase 3 trial were flown to one of two locations and housed at a hotel close to the study site. The protocol required a separate nurse (outside of the study site) to visit the patient and provide an overview of the study requirements, obtain lab samples, and check on the overall health of the patients outside of site visits. Additionally, the designated hotel was to provide 24/7 supplementary healthcare services.
During the trial, the nurse coordinator received a phone call from the sponsor. The sponsor reported it had received its first patient on placebo. The patient experienced immobility and was unable to complete any of their activities of daily living (ADLs). The patient’s caregiver was struggling to provide care for the patient. The designated hotel had stopped providing 24/7 healthcare services, unbeknownst to the sponsor. The patient was ready to withdraw from the study, desperate to stabilize symptoms by resuming the open label drug via the separate trial.
The nurse coordinator identified nursing agencies within its network that could provide 24/7 healthcare services in conjunction with the assigned home care nurse for the duration of the patient’s stay to facilitate the completion of the remaining study requirements. The sponsor, home care nurse, and nurse coordinator successfully functioned as a cohesive team to staff the patient with a private duty aide within 45 minutes of the initial phone call from the sponsor.

The patient was able to receive the care that was needed to remain on placebo and completed the remaining study requirements. The sponsor did not have to extend the recruitment period, and overall study timelines were not impacted. More importantly, the patient and caregiver needs were addressed, and the intervention positively affected their experience in participating in the trial.
3. Personalized Patient Retention Services
The third type of retention service is personalized services. Personalized services are highly individualized services that can be applied in situations when enrollment and/or retention are particularly challenging, or to maintain contact with a rare population between studies.
Personalized retention services are targeted to a participant’s interests as self-reported in a detailed survey. For instance, the patient is asked about favorite hobbies or activities (e.g., do they enjoy ballet performances, attending a baseball game, gardening, going to dinner at the mom and pop restaurant in the next town over?). A custom retention program is then designed specifically for the patient that includes only the activities they love.
An appealing aspect of a personalized retention program is the opportunity for study participants to interact socially. While this would not be acceptable during active study drug and blinding, it works well in long-term registries and observational studies. Peer support can be a strong motivator to help overcome the social isolation and impairment that are common among the chronically ill.2,3 For instance, sites can rent a movie theater and extend invitations to study participants, offering a reduced cost for a special screening complete with popcorn and candy. Another popular event option is to offer a breakfast and question and answer session with study doctors, who can personally provide study updates and medical advances regarding the disease.
These events build a sense of pride and accomplishment among participants and can help participants feel committed and appreciated.
Can Patient Services Help Conquer Your Enrollment And Retention Challenges?
Costly delays and extensions of clinical trials can be avoided when plans are in place to help study sites and patients. This approach seeks to meet the need of trial sponsors, trial sites, and the participants by understanding and accommodating the specific needs of clinical trial participants.
Visit our website: www.ubc.com.
References
1. Scientific American, “Many Pediatric Studies Are A Waste Of Time,” Charles Schmidt, September 1, 2017.
2. Tilden, V.P. and Weinert, C. (1987) Social Support and the Chronically Ill Individual. Nursing Clinics of North America, 22, 613-620.
3. Holley, U. A. (2007), Social Isolation: A Practical Guide for Nurses Assisting Clients with Chronic Illness. Rehabilitation Nursing, 32: 51–58. doi:10.1002/j.2048-7940.2007.tb00152.x

Biography
Joel Roberts leads patient recruitment, retention, and site support programs for global phase III and IV clinical studies. With a passion for science, recruitment, and emerging technologies, Joel has been at the forefront of developing innovative solutions at UBC to make it easier for people to understand and participate in research.